| |
| |
| Neurogenic Bladder |
|
|
The normal function of the bladder is to store and empty urine in a coordinated, controlled fashion. This coordinated activity is regulated by a complex interaction of the central and peripheral nervous systems. But what happens when the bladder malfunctions? This can be due to anatomic or neurologic anomalies from congenital defects, diseases or injuries. The information below will help define characteristics of a normal and abnormal bladder along with proper evaluation and management. |
| |
|
| What happens under normal conditions? |
|
|
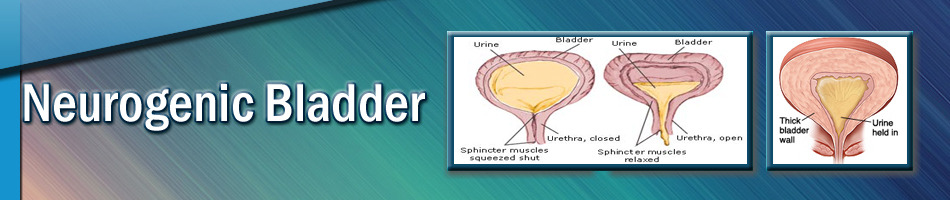
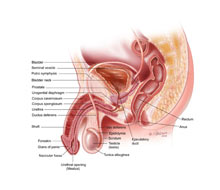
The urinary bladder is a spherical organ with unique properties that enable it to store and empty urine. The bladder is composed of two functional layers an inner urothelial lining and an outer smooth muscle layer. In addition to the bladder, the bladder neck is a funnel-like outlet of the bladder which leads to the urethra. It is also known as the internal sphincter. The urethra a tube-like structure which serves as a channel to carry urine from the bladder to the external surface, and the external urethral sphincters composed of striated muscles (group of muscles which surround the urinary passage distal to the bladder neck) complete the lower urinary tract.
The muscles and nerves of the urinary system must function in a coordinated fashion with the bladder in order to perform its two major functions of storage and elimination of urine. Nerves carry messages from the bladder to the brain and then from the brain to the muscles of the bladder telling them to tighten or release, allowing the bladder to empty during urination.
There are two main components to a normal micturition cycle of the bladder: storing and emptying. The bladder will initially fill (store urine) under a low pressure (high compliance). This requires both relaxation of the detrusor muscle along with its elastic properties of the bladder wall to enable the bladder to expand under low pressure. At the same time the striated sphincter is required to be contracted to maintain an elevated outlet resistance preventing urinary leakage. In order for the bladder to empty, the sphincter relaxes followed by a bladder contraction. Any abnormality in either component of the micturition cycle leads to bladder dysfunction. |
| |
|
| What is neurogenic bladder? |
|
|
Neurogenic bladder is the loss of normal bladder function caused by damage to part of the nervous system. The damage can cause the bladder to be underactive, in which it is unable to contract and unable to empty completely, overactive, in which it contracts to frequently without being able to be inhibited or inability to coordinate bladder contractions with sphincter relaxation (Detrusor Sphincter Dysnergey or DSD).
|
| |
|
| What are some risk factors for neurogenic bladder? |
|
|
Risk factors for neurogenic bladder include various birth defects, which adversely affect the spinal cord and function of the bladder, including spina bifida or sacral agenesis and other spinal cord abnormalities. Tumors within the spinal cord or pelvis may also disrupt normal nervous tissue function and place an individual at risk. Traumatic spinal cord injury is also a major risk factor for development of neurogenic bladder. |
| |
|
| What are the symptoms of neurogenic bladder? |
|
|
Inability to control urination, also known as urinary incontinence is associated with the neurogenic bladder. This may be caused by abnormalities in bladder capacity or malfunction of control mechanisms such as the bladder neck and/or external urethral sphincter muscle that are important for the bladder's storage function.
Symptoms including a dribbling urinary stream, straining during urination or inability to urinate may also be associated with neurogenic bladder. Urinary retention may result either from loss of bladder muscle contracting performance or loss of appropriate coordination between the bladder muscle and the external urethral sphincter muscle. In addition, symptoms of repeated UTIs or new findings of hydronephrosis (dilation of the kidneys) can be initial symptoms of a neurogenic bladder.
Increased bladder pressures from neurogenic bladders can be caused by the inability of the bladder muscle to relax properly and expand to store urine. This can be caused from the inability to coordinate relaxation of urethral sphincter with contraction (DSD) or from inability to relax urethral sphincter. Patients with increased bladder pressures are at an increased risk for UTIs and pyelonephritis along with kidney damage and even failure secondary to long standing high pressures.
Stones may also form in the urinary tract of individuals with a neurogenic bladder caused by the stoppage of urine flow and/or infection.
Abnormal backup of urine from the bladder to the kidney(s), also known as vesicoureteral reflux (VUR), may develop as a means of releasing high pressure within the bladder. A UTI is of particular concern as VUR may place the patient at significant risk for a severe kidney infection by transporting infected bladder urine directly to the kidney(s). |
| |
|
| How is neurogenic bladder diagnosed? |
|
|
When neurogenic bladder is suspected, both the nervous system (including the brain) and the bladder itself are tested. In addition to complete medical history and physical examination, diagnostic procedures may include:
Bladder function tests including Urodynamic evaluations, which has two components CMG (Cystometrogram) which measures bladder function, capacity, compliance and voiding and storage pressures. Along with EMG (Electromypography) which measures which help measure urethral sphincter tone and bladder coordination.
Radiologic imaging of the of the spine and brain including x-ray and MRI can be used
Imaging tests of the bladder and kidneys are performed
|
| |
|
| How is neurogenic bladder treated? |
|
|
The main goal of Urologic management is to prevent damage to the upper tracts (kidneys). The secondary goal is minimize any social disabilities.
Medication for treatment of overactive bladder may improve or relieve irritating symptoms and/or incontinence. Other medications may improve bladder control by increasing outlet resistance at the bladder neck.
In 1981 Dr. McGuire observed that upper tract deterioration occurred when the detrusor leak point pressure exceeded 40cm/H20 measured by Urodynamics. Detrusor sphincter dysnergy (DSD) has also been found to be a significant risk factor for upper tract deterioration. Denervation of the external sphincter can lead to a fixed open sphincter resulting in bladder outlet obstruction. Both DSD and bladder outlet obstruction leads to bladder hypertrophy and loss of bladder compliance and decrease in capacity leading to elevated bladder pressures.
Clean intermittent catheterization (CIC) was developed by Dr. Jack Lapides in the early 1970s as a means of emptying the bladder in the case of a bladder muscle that is unable to contract or in patients with loss of appropriate coordination between the bladder muscle and the external urethral sphincter muscle (DSD). The same medications used to treat bladder over activity (anticholinergic medications) are used to help improve bladder storage pressures.
There have been numerous studies demonstrating that aggressive early management with patients with neurogenic bladders at high risk (patients with DSD or elevated bladder pressures) with CIC and anticholinergic medications have lead to decrease upper tract deterioration (kidney damage and failure) along with decreased need for future bladder augmentation surgery.
Surgical cutting or dilation of the external urethral sphincter with the use of an endoscope passed through the urethra and can eliminate the need for CIC in order to empty the bladder but at the expense of total urinary incontinence and frequently is only temporary.
At times, however, damage to bladder anatomy and function is so severe that capacity needs to be improved with bladder augmentation (increasing bladder size with various tissues), vesicoureteral reflux needs to be corrected and/or an alternate tube (catheterizable channel) for emptying the bladder may need to be surgically constructed for patients that are unable to catheterize through their urethras.
|
| |
|
| What can be expected after treatment for neurogenic bladder? |
|
|
A person can expect extensive follow-up evaluation of bladder and kidney function. This may involve repeated X-rays, ultrasound, blood tests and bladder function tests.
Although some characteristics of the neurogenic bladder may improve or resolve, most issues typically require constant attention and reevaluation.
Proactive management of patients with a neurogenic bladder may decrease the risk of damage to the bladder and kidney(s) and, therefore, potentially limit the need for future intervention. This has been shown in management of neurogenic bladder patients with spina bifida.
|
| |
|
Frequently asked questions:
What is the likelihood that my child with spina bifida will develop neurogenic bladder? |
|
|
The risk of neurogenic bladder is significant in this population and, therefore, careful and frequent evaluation of bladder function is recommended.
|
| |
|
| What are expected limitations for a patient with neurogenic bladder? |
|
|
Limits are typically a function of the cause of neurogenic bladder (such as spinal cord injury, for example), rather than the neurogenic bladder itself. With proactive management and close medical follow-up, patients with neurogenic bladders can expect to be both socially continent of urine along with preservation of renal function.
|
| |
|
| Can the effects of a neurogenic bladder be prevented? |
|
|
Some effects of neurogenic bladder are preventable with aggressive management with medication and at times appropriate surgical reconstruction
|
| |
|
| |
| |
|
|